Information Effect Project
Death with dignity
Death with dignity is deciding when it is morally or ethically right to end one’s life due to terminally ill causes. Some of the few reasons this topic holds controversy is due to the fact that the topic itself presents an oxymoron specifically for Physicians. For them to be assisting in the end of one’s life while at the same time trying to save and overall prevent an individual from death. Many religious views also play a role in its pursuit to become legalized in more states in the U.S. When you think of who has the power to make it become a citizen right, if it against ones belief it can be a tenacious detriment to society. Oregon was one of the first six states to have legalized the death with dignity act. The following individual shares her story of being able to take advantage of how being able to make a choice for her life, gave her a better life.
Death with dignity is deciding when it is morally or ethically right to end one’s life due to terminally ill causes. Some of the few reasons this topic holds controversy is due to the fact that the topic itself presents an oxymoron specifically for Physicians. For them to be assisting in the end of one’s life while at the same time trying to save and overall prevent an individual from death. Many religious views also play a role in its pursuit to become legalized in more states in the U.S. When you think of who has the power to make it become a citizen right, if it against ones belief it can be a tenacious detriment to society. Oregon was one of the first six states to have legalized the death with dignity act. The following individual shares her story of being able to take advantage of how being able to make a choice for her life, gave her a better life.
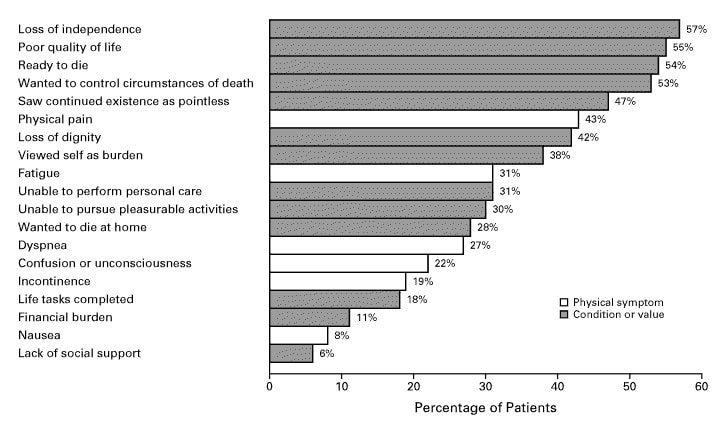
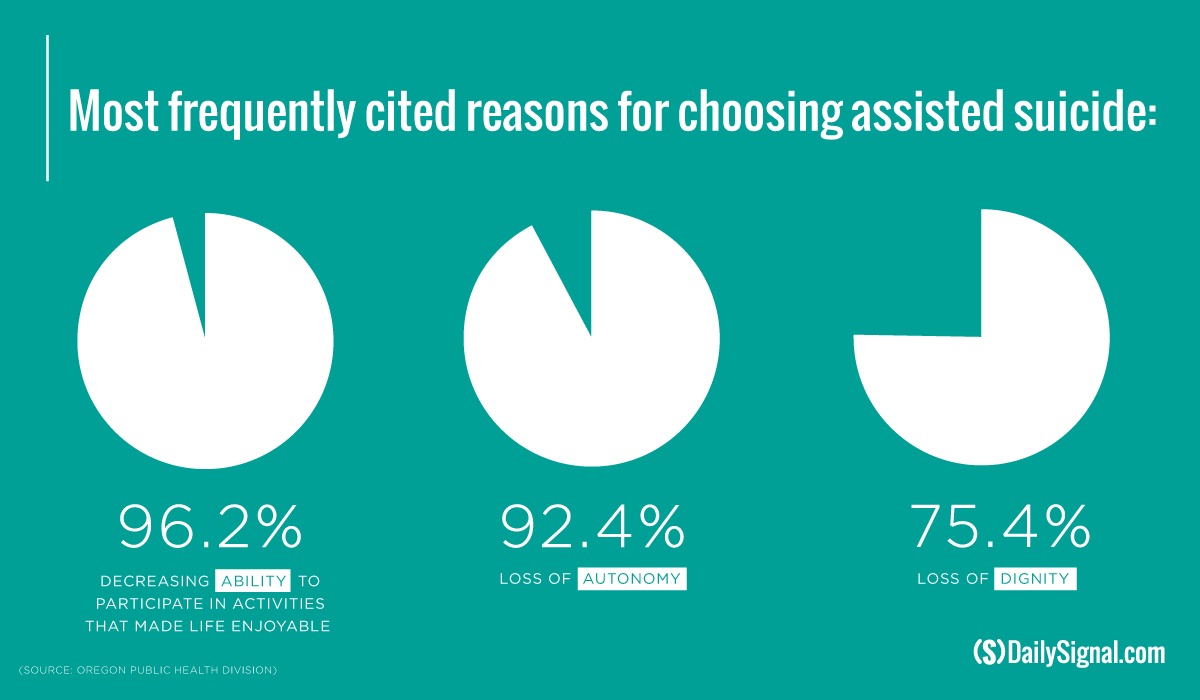
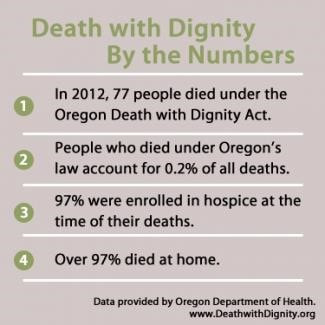
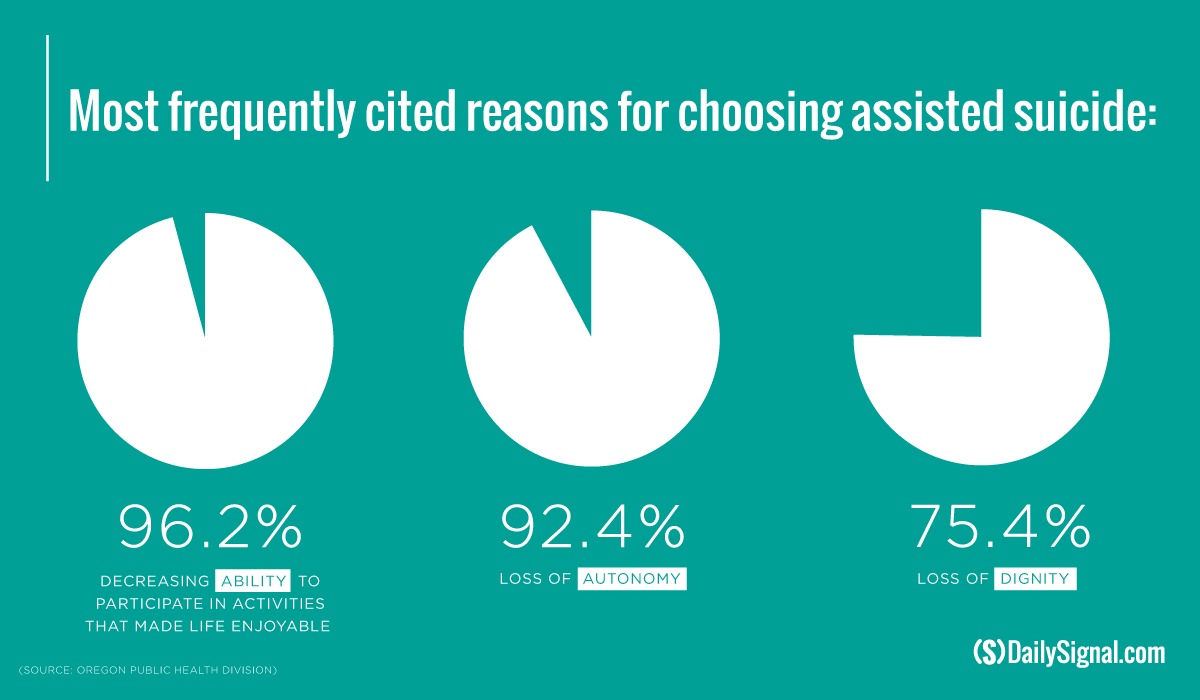
Brittany Maynard, was a 29 year old women who lived in California suffering from terminal brain cancer. She goes on to explain how her and her family’s life turned into hospital stays. After several doctor visits and medical research being conducted, Brittany had two surgeries done to try and prevent the spread of her brain tumor. It wasn't until later that year Brittany and her family had learned that not only her tumor grew back, but bigger and more aggressive than before. The treatment recommended by doctors was full brain radiation, which the side effects are consisted of extreme hair loss and first degree burns covering her scalp. After months of hope and research the Maynards were able to come to the conclusion that there is no solution to save Brittany's life only solutions to temporarily prolong her life. Brittany considered passing away at a home hospice care center near the San Francisco Bay area near where she lived. Brittany and her family decided that hospice care would provide palliative care that could worsen her physical and mental state of mind and that is not how Brittany wanted her family to remember her as. Below is a chart further explaining examples of patients choices as to why they chose to take advantage of physician assisted suicide due to the burdens that were carried with terminal illnesses.
Brittany had been married only for a year before being diagnosed and told she had six months to live. Regarding the death with dignity act, it stipulates that a patient can only take advantage of death with dignity act if they have been diagnosed with only six months to live. Brittany contemplated the choices she had and decided to look further into death with dignity and came to the conclusion that would be the best scenario for her. At the time the state of California had not yet enacted their death with dignity act, Maynard and her family did what they found best and moved to the state of Oregon to take advantage of their legal death with dignity law which was one of the only five state to have legalized this option. After establishing residency in Oregon, Brittany was able to get approved for her self-medication which when life became too physically unbearable she could choose to end it on her own terms. She claims “I am not suicidal. If I were I would have consumed that medication long ago. I do not want to die, but I am dying and I want to die on my own terms.” She also went on to say “I would not tell anyone else that he or she should choose death with dignity. My question is: Who has the right to tell me that I don't deserve this choice? That I deserve to suffer for weeks or months in tremendous amounts of physical and emotional pain? Why should anyone have the right to make that choice for me?” Having this choice gave tremendous amounts of relief to Brittany. It gave her the ability to live her day to day life knowing she had a safety net. It was on November 1st, 2014 Brittany Maynard decided to end her life in Oregon. At the time she was beginning to suffer from severe seizures that would lead to neck pain that would inhibit her ability to speak. Since Oregon’s choice of their death with dignity act up until December 31st, 2013 more than 750 people have taken advantage over their death with dignity act. The median age group for this was at about the age of 71, only six of that 750 were below the age of 35 such as Maynard. Brittany became a volunteer leading advocate for the nation’s leading end of life choice at the compassion and choices organization. Learn more about her Brittany and her family’s story at www.thebrittanyfund.org
Religion and Spirituality
When we talk about how religion plays a role in death with dignity and in a story such as Brittany Maynard, Janet Morana, a director for the group Priests for Life, had the following to say after Maynard's passing. "We are saddened by the fact that this young woman gave up hope, and now our concern is for other people with terminal illnesses who may contemplate following her example. Our prayer is that these people will find the courage to live every day to the fullest until God calls them home. Brittany's death was not a victory for a political cause. It was a tragedy, hastened by despair and aided by the culture of death invading our country." When we talk about religion and spirituality regarding death with dignity it tends to stir some controversy when the two topics collide. Here is where the following religions stand and have to say about one’s choice in ending their own life. For Baptist and Southern Baptist churches their statement claims “to advocate within the medical community for increased emphasis on the caring goals of medicine which preserve the dignity and minimize the suffering of the individual and respect personal choice for end of life care.” Unlike Baptists views Roman Catholic view are much stricter when it comes to their view on the subject. They claim that the killing of a human being violates divine law and offends the dignity of the human person. Pope Benedict XVI has come forward to say that physician aid in dying shows “false compassion” and the action results in “devaluing and dehumanizing the sick”. Which is what he claims all to be considered is our “throwaway culture.” LDS views come to say that suicide violates the commandments of God although the church does recognize that when a person is in their final stages of terminal illness there may be difficult decisions to make. “When dying becomes inevitable, death should be looked upon as a blessing and a purposeful part of an eternal existence. Members should not feel obligated to extend mortal life by means that are unreasonable.” For the majority the opinion being held all appeals to the same answer just presented a different way. Some may not be particularly clear on which side they stand on while others have a more solid idea of what they believe in.
Physicians Point of View
Take a look at Physician assisted suicide from the perspective from that of several Physicians. From Oregon’s Physicians, since the law became enacted of October 27th, 1997 a survey was conducted from physicians living within the state of Oregon to answer questions about their patients who had made requests for Physician assisted suicide. The survey was able to identify with one hundred and forty four respondents to the survey. From that number they were able to conclude that the physicians had received 221 requests for lethal medication. From there the physicians were to answer more questions regarding their patient’s characteristics. The median age of request at this time was around the age of 68, and the most common cause of the terminal illness was cancer.
Religion and Spirituality
When we talk about how religion plays a role in death with dignity and in a story such as Brittany Maynard, Janet Morana, a director for the group Priests for Life, had the following to say after Maynard's passing. "We are saddened by the fact that this young woman gave up hope, and now our concern is for other people with terminal illnesses who may contemplate following her example. Our prayer is that these people will find the courage to live every day to the fullest until God calls them home. Brittany's death was not a victory for a political cause. It was a tragedy, hastened by despair and aided by the culture of death invading our country." When we talk about religion and spirituality regarding death with dignity it tends to stir some controversy when the two topics collide. Here is where the following religions stand and have to say about one’s choice in ending their own life. For Baptist and Southern Baptist churches their statement claims “to advocate within the medical community for increased emphasis on the caring goals of medicine which preserve the dignity and minimize the suffering of the individual and respect personal choice for end of life care.” Unlike Baptists views Roman Catholic view are much stricter when it comes to their view on the subject. They claim that the killing of a human being violates divine law and offends the dignity of the human person. Pope Benedict XVI has come forward to say that physician aid in dying shows “false compassion” and the action results in “devaluing and dehumanizing the sick”. Which is what he claims all to be considered is our “throwaway culture.” LDS views come to say that suicide violates the commandments of God although the church does recognize that when a person is in their final stages of terminal illness there may be difficult decisions to make. “When dying becomes inevitable, death should be looked upon as a blessing and a purposeful part of an eternal existence. Members should not feel obligated to extend mortal life by means that are unreasonable.” For the majority the opinion being held all appeals to the same answer just presented a different way. Some may not be particularly clear on which side they stand on while others have a more solid idea of what they believe in.
Physicians Point of View
Take a look at Physician assisted suicide from the perspective from that of several Physicians. From Oregon’s Physicians, since the law became enacted of October 27th, 1997 a survey was conducted from physicians living within the state of Oregon to answer questions about their patients who had made requests for Physician assisted suicide. The survey was able to identify with one hundred and forty four respondents to the survey. From that number they were able to conclude that the physicians had received 221 requests for lethal medication. From there the physicians were to answer more questions regarding their patient’s characteristics. The median age of request at this time was around the age of 68, and the most common cause of the terminal illness was cancer.
Fifty-nine percent of the Physicians who responded to the survey who practiced in small towns supported the law, but physicians in small towns were unlikely to prescribe lethal medication as well as if the patient viewed themselves as a burden to others or suffered from depression. Doctors state that a patients request is more likely to be honored if they are enrolled in a hospice care program and or wanted to control the manner of their death if it were a terminal illness such as cancer. Some of the problems that Physicians reported having with the assistance of someone’s death was having unwanted publicity, having a hard time obtaining the lethal medication or gathering a second opinion, difficulty understanding the requirements of the law at the time and everything it entailed. Four physicians expressed ambivalence about having provided assistance with suicide, though two of the four noted that they had become less ambivalent over time. One of these physicians decided not to provide such assistance again.

We may never be able to come to a conclusion about who is right and who is wrong. Being able to draw a fine line between someone else’s choice of life and if they have that decision to make themselves can be difficult to address. Needless to say that is not what death and dignity is about. Each situation can be different and should be addressed as such, a constant evaluation followed by a system of stipulations. Consider the many points of view there are, evaluate them and come to a consensus. Take Maynards story for example, and the many details to examine. Consideration of religious views of some that may inhibit ones decision and a Physicians professional view as to whether they support or do not support the idea.
Can you afford to die?
Since Oregon’s enactment of the death with dignity act in October of 1997, Oregon has
become the first state to enact Physician Assisted Death (PAD). It has now been over 20 years
and this topic still seems to hold a good amount of controversy to its name. As of February 20,
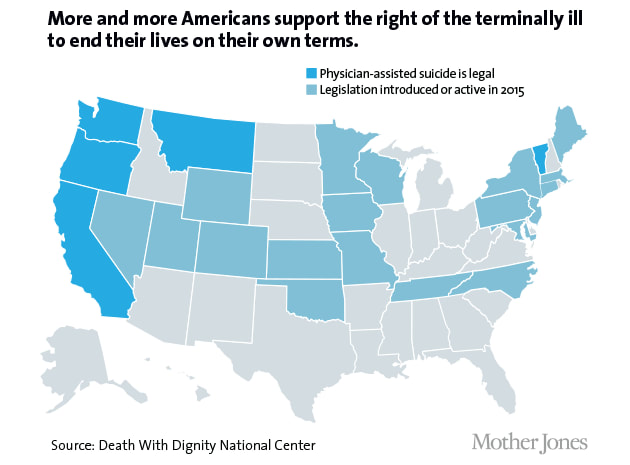
2017, the states of Oregon, Washington, California, Colorado, District of Columbia, and
Vermont all have death with dignity laws intact. While along this road we have observed that
seven out of ten Americans that support death with dignity, but due to religious views, ethics and
moral, and the oxymoron this topic holds, we still seem unable to draw to a conclusion about if
it’s an acceptable terms of one’s choice of life. At some point everyone here will come to a point
where death will approach you. It is inevitable, a universally accepted part of life. Now let’s say
when that time comes, you are not allowed to choose when, or how that happens being that you
become incapable.
Since Oregon’s enactment of the death with dignity act in October of 1997, Oregon has
become the first state to enact Physician Assisted Death (PAD). It has now been over 20 years
and this topic still seems to hold a good amount of controversy to its name. As of February 20,
2017, the states of Oregon, Washington, California, Colorado, District of Columbia, and
Vermont all have death with dignity laws intact. While along this road we have observed that
seven out of ten Americans that support death with dignity, but due to religious views, ethics and
moral, and the oxymoron this topic holds, we still seem unable to draw to a conclusion about if
it’s an acceptable terms of one’s choice of life. At some point everyone here will come to a point
where death will approach you. It is inevitable, a universally accepted part of life. Now let’s say
when that time comes, you are not allowed to choose when, or how that happens being that you
become incapable.
Logical:
Now wouldn’t it be logical that if someone is on life support or unable to perform day to
day tasks would want to make a more dignified exit? Let’s bring this down to scale on a simpler
view. We as humans make the decision of life or death when it comes to animals. We decide
what deems acceptable for an animal to pursue a potentially good life and not. So when it comes
to humans what makes it different? What values and metrics do we measure our lives to make
another’s life livable by our standards? Can you see where this may seem selfish? My values or
standards should determine what is acceptable for another person’s will to live. When the quality
of someone’s life degrades, they should be the ones to decide how they would like to be
remember as. Dignified. In an act of war if a solider found another soldier lying on the ground
suffering they would have to decide in that exact moment what decision to make.
Now wouldn’t it be logical that if someone is on life support or unable to perform day to
day tasks would want to make a more dignified exit? Let’s bring this down to scale on a simpler
view. We as humans make the decision of life or death when it comes to animals. We decide
what deems acceptable for an animal to pursue a potentially good life and not. So when it comes
to humans what makes it different? What values and metrics do we measure our lives to make
another’s life livable by our standards? Can you see where this may seem selfish? My values or
standards should determine what is acceptable for another person’s will to live. When the quality
of someone’s life degrades, they should be the ones to decide how they would like to be
remember as. Dignified. In an act of war if a solider found another soldier lying on the ground
suffering they would have to decide in that exact moment what decision to make.
Reasonable:
What would be reasonable to consider in a situation is the potential “what if?” What if we
just need to pull through the hard times and maybe PAD wouldn’t be necessary? True, life is
something that shouldn’t be taken lightly, in a literal life or death situation we shouldn’t be quick
to diagnose that someone deserves the right to dignify their death. Terminally ill patients may
often experience depression as a side effect, therefore making them mentally unable to make this
decision considering that depression can be treated. Also palliative care is an example of how
pain is controllable and can be dealt with. The oxymoron this controversy rings is that why
would a physician, one who is intended to be there to help others heal and recover chose to do
the opposite of what their whole career entails? Irony in life and death.
What would be reasonable to consider in a situation is the potential “what if?” What if we
just need to pull through the hard times and maybe PAD wouldn’t be necessary? True, life is
something that shouldn’t be taken lightly, in a literal life or death situation we shouldn’t be quick
to diagnose that someone deserves the right to dignify their death. Terminally ill patients may
often experience depression as a side effect, therefore making them mentally unable to make this
decision considering that depression can be treated. Also palliative care is an example of how
pain is controllable and can be dealt with. The oxymoron this controversy rings is that why
would a physician, one who is intended to be there to help others heal and recover chose to do
the opposite of what their whole career entails? Irony in life and death.
The Process:
There are many points of view to consider when observing death with dignity as a whole.
The motive or mental state of a patient. As the quality of life starts to deteriorate so does the
mental state of that person. Would it be ethical to allow that patient to make a life or death
decision when they are not under the right circumstances to be making such a drastic decision?
Their decision may be influenced by something greater than the terminal illness itself. First off,
the requirements for a patient to enroll in their assisted suicide involves the following: Two oral
requests and one written request with their doctor treating their terminal illness as well as a
mental evaluation with a mental health professional if the doctor feels as though the patients
mental state is impairing their decision.
Consider the costs:
Consider the costs to sustain life with a terminal illness at a traditional hospital in
comparison to at home hospice care. Let’s consider the options. Palliative care serves as a
temporary, but more comforting solution. Its purpose serves to relive pain without having to deal
with the condition from which the pain stems from. For example: A patient with excruciating,
debilitating back pain could oversee countless surgeries, with the possibility of no success could
then resort to Palliative care. This would provide relief for the pain and give a more comfortable
way of living temporarily. Although some may argue this may only promote opioid addiction in
some cases, if the problem proceeds to be a lifelong issue/ illness the patient should be then
recommended to a natural or more adaptive way of living. Palliative care provides a more stress
relieving, chosen conclusion by the patient, not a hospital. “Home hospice care saves between 31
and 64 percent of medical care costs22-27.” The majority of these savings comes from tests and
hospital services that are not needed with at home hospice care. During the last six months of life, the mean medical costs for patients receiving hospice care at home are 27 percent less than for conventional care, and the savings with hospital-based hospice care are less than 15 percent22,24,26. Treatment to prolong
a terminal illness would provide a longer quantity of life, but degrade the quality of life. Giving
palliative care would give some relief, but the question is for how long? When and who decides
when enough is enough? If at home hospice care is really saving any money as opposed to
traditional hospitals. Whether or not the terminal illness was self-inflicted meaning, heart failure
from obesity, lung cancer from smoking, or kidney failure from alcoholism. These are all very
reasonable hypotheticals and should come into question when pondering if patients from such
deserve the choice in the conclusion of one’s life.
There are many points of view to consider when observing death with dignity as a whole.
The motive or mental state of a patient. As the quality of life starts to deteriorate so does the
mental state of that person. Would it be ethical to allow that patient to make a life or death
decision when they are not under the right circumstances to be making such a drastic decision?
Their decision may be influenced by something greater than the terminal illness itself. First off,
the requirements for a patient to enroll in their assisted suicide involves the following: Two oral
requests and one written request with their doctor treating their terminal illness as well as a
mental evaluation with a mental health professional if the doctor feels as though the patients
mental state is impairing their decision.
Consider the costs:
Consider the costs to sustain life with a terminal illness at a traditional hospital in
comparison to at home hospice care. Let’s consider the options. Palliative care serves as a
temporary, but more comforting solution. Its purpose serves to relive pain without having to deal
with the condition from which the pain stems from. For example: A patient with excruciating,
debilitating back pain could oversee countless surgeries, with the possibility of no success could
then resort to Palliative care. This would provide relief for the pain and give a more comfortable
way of living temporarily. Although some may argue this may only promote opioid addiction in
some cases, if the problem proceeds to be a lifelong issue/ illness the patient should be then
recommended to a natural or more adaptive way of living. Palliative care provides a more stress
relieving, chosen conclusion by the patient, not a hospital. “Home hospice care saves between 31
and 64 percent of medical care costs22-27.” The majority of these savings comes from tests and
hospital services that are not needed with at home hospice care. During the last six months of life, the mean medical costs for patients receiving hospice care at home are 27 percent less than for conventional care, and the savings with hospital-based hospice care are less than 15 percent22,24,26. Treatment to prolong
a terminal illness would provide a longer quantity of life, but degrade the quality of life. Giving
palliative care would give some relief, but the question is for how long? When and who decides
when enough is enough? If at home hospice care is really saving any money as opposed to
traditional hospitals. Whether or not the terminal illness was self-inflicted meaning, heart failure
from obesity, lung cancer from smoking, or kidney failure from alcoholism. These are all very
reasonable hypotheticals and should come into question when pondering if patients from such
deserve the choice in the conclusion of one’s life.

In retrospect, considering all options from both logical and reasonable point of views.
From past events led up until now. Physician assisted death is a topic that shouldn’t be taken
lightly. I feel though all aspects of one’s situation may vary from one person onto another
making it difficult to come to one conclusion that suits all. Overall, a patient should have the
choice to make for their own personal health. Just as we do when we decide to receive help for
an illness. It is important that a patient feels that they have options even if it is assistance in one’s
death. Palliative or hospice care is only temporarily relieving some of the pain. While from a
psychological standpoint there are stipulations in place to prevent one from choosing assistance
in their death if their mental states impairs their decision. I believe that another person’s opinion
should not prevent another person from making a personal choice for themselves when it
involves their health.
From past events led up until now. Physician assisted death is a topic that shouldn’t be taken
lightly. I feel though all aspects of one’s situation may vary from one person onto another
making it difficult to come to one conclusion that suits all. Overall, a patient should have the
choice to make for their own personal health. Just as we do when we decide to receive help for
an illness. It is important that a patient feels that they have options even if it is assistance in one’s
death. Palliative or hospice care is only temporarily relieving some of the pain. While from a
psychological standpoint there are stipulations in place to prevent one from choosing assistance
in their death if their mental states impairs their decision. I believe that another person’s opinion
should not prevent another person from making a personal choice for themselves when it
involves their health.

Adaptation Creative non fiction
The Dying Musician
Striving for greatness, a musician’s life isn’t always easy. Think of something you’re good at. Now think of when you very first started that. My uncle Carl worked hard to be to the level he did when it came to the role of a musician. He played his guitar like it was of second nature to him. He held his guitar with this aggressive grip, almost as if he would throw it into the crowd when he finished playing at a show. It was hard to read the emotion of his actions. Almost as if he was angry or just really passionate about his music.
When I was only 12 years old my uncle was a role model for me and led me to buying my very first guitar. On the voyeur to the many stores in search for my prized possession. He had helped me to purchase my guitar once we had first found it. I was beyond grateful and ambitious to begin playing.
Do you ever ask someone that question that always follows with the same answer every time? “How are you doing Carl?” The same “I’m fine” answer was always enough for everyone else. Even still today we celebrate his personality, his love for music and family outings. I still have my guitar and pick it up from time to time and when I do I still think of the first time I heard him play. I think of how all of his things are still kept still. Like an abandoned room that never lost its meaning
I remember his brother quoting at the time of his passing; “Now the hardness of this world, slowly grinds your dreams away. Making a fool’s joke out of the promises we make and what once seems black and white turns to so many shades of gray. So we lose ourselves in work to do and bills to pay and it’s a ride, ride, ride, and there ain’t much cover with no one running by your side, my blood brother.” –Bruce Springsteen.
The Dying Musician
Striving for greatness, a musician’s life isn’t always easy. Think of something you’re good at. Now think of when you very first started that. My uncle Carl worked hard to be to the level he did when it came to the role of a musician. He played his guitar like it was of second nature to him. He held his guitar with this aggressive grip, almost as if he would throw it into the crowd when he finished playing at a show. It was hard to read the emotion of his actions. Almost as if he was angry or just really passionate about his music.
When I was only 12 years old my uncle was a role model for me and led me to buying my very first guitar. On the voyeur to the many stores in search for my prized possession. He had helped me to purchase my guitar once we had first found it. I was beyond grateful and ambitious to begin playing.
Do you ever ask someone that question that always follows with the same answer every time? “How are you doing Carl?” The same “I’m fine” answer was always enough for everyone else. Even still today we celebrate his personality, his love for music and family outings. I still have my guitar and pick it up from time to time and when I do I still think of the first time I heard him play. I think of how all of his things are still kept still. Like an abandoned room that never lost its meaning
I remember his brother quoting at the time of his passing; “Now the hardness of this world, slowly grinds your dreams away. Making a fool’s joke out of the promises we make and what once seems black and white turns to so many shades of gray. So we lose ourselves in work to do and bills to pay and it’s a ride, ride, ride, and there ain’t much cover with no one running by your side, my blood brother.” –Bruce Springsteen.
